
More Information
Submitted: October 31, 2023 | Approved: November 27, 2023 | Published: November 28, 2023
How to cite this article: Kucukakcali Z, Cicek IB. To Examine the Effects of Risk Factors Associated with Kidney Stones in Determining the Disease by Considering their Combinations. Arch Surg Clin Res. 2023; 7: 046-051.
DOI: 10.29328/journal.ascr.1001073
Copyright License: © Kucukakcali Z, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Kidney stone; Variable combination; Diagnosis

To Examine the Effects of Risk Factors Associated with Kidney Stones in Determining the Disease by Considering their Combinations
Zeynep Kucukakcali* and Ipek Balikci Cicek
Department of Biostatistics and Medical Informatics, Inonu University Faculty of Medicine, 44280, Malatya, Turkey
*Address for Correspondence: Zeynep Kucukakcali, Department of Biostatistics and Medical Informatics, Inonu University Faculty of Medicine, 44280, Malatya, Turkey, Email: [email protected]
Aim: Kidney stone disease, which can affect people of all ages and whose incidence increases day by day, is becoming a public health problem due to treatment costs. This study aims to determine how factors related to kidney stones affect the diagnosis of the disease when taken together, rather than determining their relationship with the disease one by one.
Materials and methods: An open-access dataset containing kidney stone status and associated factors was used in the study. Mann Whitney U test and independent sample t-test were used in data analysis. Logistic regression was performed with the backward variable selection method to determine the factors associated with kidney stones. ROC analysis was used to determine the power of the variables that were significant as a result of logistic regression analysis, individually and together, in discriminating kidney stones.
Results: According to the results of logistic regression analysis, gravity, cond, and urea calc variables were found to be associated with kidney stones. With ROC analysis, it can be said that urea, calc, and gravity variables with AUC values above 0.60 can distinguish kidney stones. When the combinations of these variables are examined, the AUC values of the binary combinations are between 0.734 and 0.759, while the AUC value obtained for the triple combination is 0.831.
Conclusion: According to the results obtained from the article, it can be said that while the factors associated with the disease and used in the diagnosis have little effect on the diagnosis of the disease alone based on the AUC values obtained from the ROC analysis, it can be said that considering them together increases the accuracy in diagnosis. Therefore, considering the factors thought to be associated with the disease together may be more appropriate in diagnosis and may give more accurate results.
Kidney stone disease, commonly known as nephrolithiasis or urolithiasis, is one of medicine's oldest disorders. It is predicted that 1% - 15% of people may get kidney stones at some point in their lives, and the prevalence and incidence of kidney stones are increasing globally [1-4]. According to a recent study conducted in China, the prevalence of kidney stones was stated to be 5.8% among Chinese adults (6.5% in men and 5.1% in women), and it was concluded that 1 in every 17 adults is affected by kidney stone disease [5,6]. It causes about 80,000 hospitalizations in the UK each year, and data from the United States show that its prevalence has risen from 3.8% in 1976-1980 to 8.8% in 2007-2010 [7,8]. As a result, the prevalence of kidney stone disease, which varies from region to region, has been increasing day by day in the last 30-40 years. For this reason, it has become one of the most common diseases today and has become an important public health problem, resulting in serious treatment costs. Without adequate treatment, kidney stones can cause ureter obstruction, blood in the urine, recurrent urinary tract infections, vomiting, or painful urination, resulting in irreversible functional impairment to the kidneys [9,10]. Urolithiasis is frequently a recurring and lifelong condition, with a 50% recurrence rate after 5-10 years and a 75% recurrence rate within 20 years [11,12].
In light of some studies, it has been shown that in addition to global warming, there is an increase in kidney stone formation due to many environmental factors such as recent changes in lifestyle and eating habits [3,10,13]. However, as mentioned, the exact factors responsible for the increasing prevalence and recurrence of kidney stone disease have not yet been identified. Kidney stone disease has a significant impact on the economy in terms of individual, community, and treatment burden due to its high prevalence in adults, especially in the working population [14]. It is becoming a major public health problem, especially in communities living in hot and dry climates where it is most common.
Therefore, there is a need for parameters that can be associated with the disease and can be used in the diagnosis of kidney stone disease, which obstructs the urinary system, leading to a decrease in quality of life and progressing to renal failure in patients, in order to predict its formation in advance and to minimize the recurrence of kidney stones.
There are many parameters associated with the diagnosis of kidney stones. Although each of these parameters is used to explain kidney stone formation, the use of each of them individually may sometimes be insufficient to explain the disease. Considering some parameters together and associating them with each other may be more effective in the diagnosis of the disease. For this purpose, in this study, the combinations of the parameters determined to be associated with renal failure will be examined and associated with kidney stones and how the evaluation of the parameters together will affect the diagnosis will be examined.
Data set and features
The dataset used in the study is a dataset consisting of clinical data of individuals with and without kidney stones. This dataset was obtained from "https://www.kaggle.com/datasets/harshghadiya/kidneystone/data" and is an open-access dataset. The kidney-stone-dataset.csv is a comma-separated values file containing data on patients with kidney stones. The file has 90 rows and 7 columns, with each row representing a patient and each column providing information on various characteristics and laboratory test results. The dataset also includes a target variable, "Risk of Stone", which is a continuous variable representing the risk of developing kidney stones. This dataset can be used for tasks such as predicting the risk of kidney stones based on patient characteristics and test results. The explanatory variables ph, osmo, urea, calc, gravity, and cond were included to explain the target variable. Explanations of explanatory variables are given below.
Gravity: It refers to urine-specific gravity, which measures the concentration of dissolved substances in urine.
pH: pH measures the acidity or alkalinity of urine.
Osmo (Osmolality): Osmolality measures the concentration of solutes (particles) in urine.
Cond (Conductivity): It measures the ability of urine to conduct electricity, which is influenced by the concentration of ions in the urine.
Urea: Urea is a waste product produced by the liver as a result of protein metabolism.
Calc (Calcium): Calcium is an important mineral that plays a role in bone health, muscle function, and nerve transmission.
Biostatistical analysis
The statistical analysis section describes the methods and tools used to analyze the data collected in the study. The data are quantitative, i.e. numerical, and measured on a scale. The conformity of the data to a normal distribution was checked with the Shapiro-Wilk test. Some of the data were normally distributed while some were not. Therefore, the normally distributed data are summarized with mean ± sd, while the non-normally distributed data are summarized with median (95% confidence interval for median). Depending on the data distribution, an independent sample t - test or Mann-Whitney U - test was used for statistical analysis. P < 0.05 was considered statistically significant.
Logistic regression analysis was performed using the backward variable selection method to determine the odds ratio of the variables. With this analysis, Hosmer & Lemeshow's goodness of fit test and omnibus test of model coefficients were calculated.
ROC analysis was performed to determine the extent to which the explanatory variables discriminate the target variable. ROC analysis was performed with the variables obtained as significant in the logistic regression model. As a result of the ROC analysis, combinations of variables with good discrimination properties were taken to determine the percentages of discrimination of the target variable. Therefore, binary logistic regression was applied to calculate the predictive probability of the combined variables for kidney stone diagnosis. ROC curves were constructed using the predictive probability as a covariate. The areas under the curves (AUCs) were used to assess the diagnostic value of the combination of each variable.
Descriptive statistics of the variables used to determine the presence/absence of kidney stones, which is the target variable in the study, are given in Table 1.
| Table 1: Descriptive statistics of explanatory variables. | |
| Variables | Median (95% confidence interval for median) |
| ph | 5.94(5.73-0.075) |
| osmo | 567(516-25.382) |
| urea | 224(195-14.278) |
| calc | 3.3(2.36-0.321) |
| Mean ± sd | |
| gravity | 1.018 ± 0.007 |
| cond | 20.696 ± 7.665 |
| Sd: standard deviation | |
The descriptive statistics of the independent variables according to the categories of the target variable and the statistical results of the tests on whether there is a statistically significant difference in the variables in terms of categories are given in Table 2.
| Table 2: Descriptive statistics and test results for categories of the target variable. | |||||
| Variables | Absence of kidney stones | Presence of kidney stones | p | ||
| Mean ± sd | Median (95% confidence interval for median) | Mean ± sd | Median (95% confidence interval for median) | ||
| gravity | 1.015 ± 0.006 | 1.017(1.015-1.02) | 1.02 ± 0.007 | 1.021(1.018-1.024) | < 0.001* |
| ph | 6.126 ± 0.686 | 5.975(5.68-6.35) | 5.975 ± 0.724 | 5.86(5.58-6.13) | 0.271** |
| osmo | 561.659 ± 234.58 | 562(450-680) | 639.378 ± 240.503 | 594(487-774) | 0.126* |
| cond | 20.55 ± 8.852 | 21.4(15.5-25.3) | 20.839 ± 6.395 | 21.382(19.8-23.6) | 0.861* |
| urea | 232.432 ± 120.02 | 219(159-284) | 279.289 ± 145.259 | 255(197-364) | 0.101* |
| calc | 2.629 ± 1.884 | 2.09(1.45-2.66) | 5.411 ± 3.311 | 5.775(4.18-6.96) | < 0.001** |
| *:Independent sample t - test; **:Mann Whitney U - test | |||||
According to the logistic regression analysis using the backward variable selection method, among the variables ph, osmo, urea, calc, gravity, and cond, are statistically significant and are explanatory variables for kidney stone status. The results of the logistic regression analysis are given in Table 3.
| Table 3: The results of the logistic regression analysis. | ||||||
| Variables | B | Wald | Sig. | Exp(B) | 95% CI for EXP(B) | |
| Lower | Upper | |||||
| gravity | 469.549 | 10.498 | 0.001 | 8.36 | 3.70 | 13.48 |
| cond | -0.180 | 8.754 | 0.003 | 0.836 | 0.742 | 0.941 |
| urea | -0.018 | 7.863 | 0.005 | 0.982 | 0.969 | 0.994 |
| calc | 0.678 | 13.210 | 0.000 | 1.971 | 1.367 | 2.841 |
| Constant | -471.759 | 10.534 | 0.001 | 0.000 | ||
According to the results obtained from logistic regression analysis, p < 0.05 for gravity, cond, urea, and calc variables, and these variables are considered risk factors for kidney stones. It is said that an increase in gravity and calc variables increases the risk of kidney stones (8.36 fold and 1.971 fold, respectively).
The results of the ROC analysis with the variables that were significant according to the logistic regression analysis results are given in Figure 1 and Table 4.
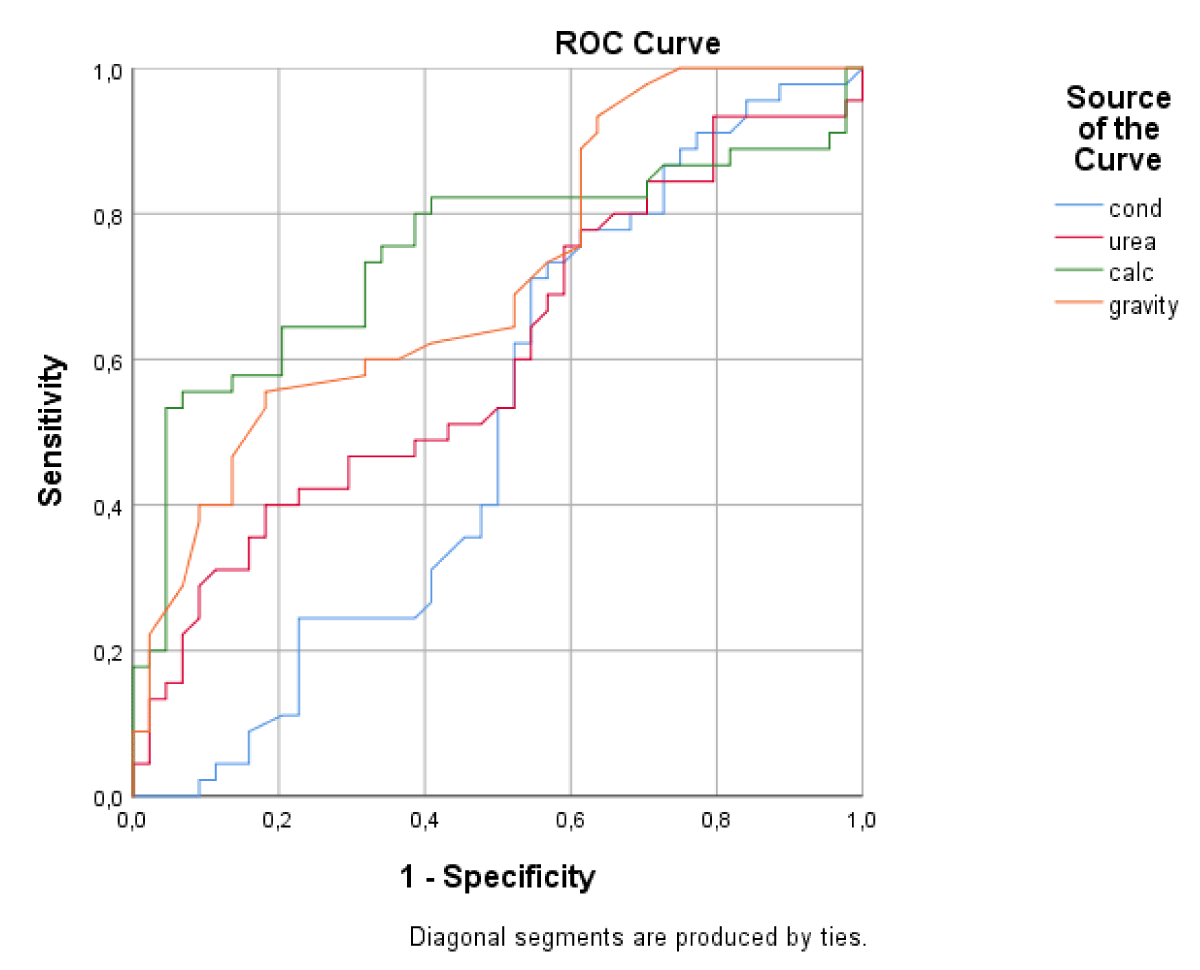
Figure 1: Graph of ROC analysis results.
| Table 4: Result of ROC analysis. | |
| Test Result Variable(s) | Area Under the Curve (AUC) |
| cond | 0.509 |
| urea | 0.602 |
| calc | 0.746 |
| gravity | 0.713 |
When the results of the ROC analysis are analyzed, it is seen that the cond variable could not distinguish the categories of the kidney stone variable, which is the target variable, and the other variables provided distinction.
According to the results of ROC analysis, the results of ROC analysis using the combinations of urea, calc, and gravity variables which are successful in discriminating the categories of kidney stone variables are given in Figure 2 and Table 5.
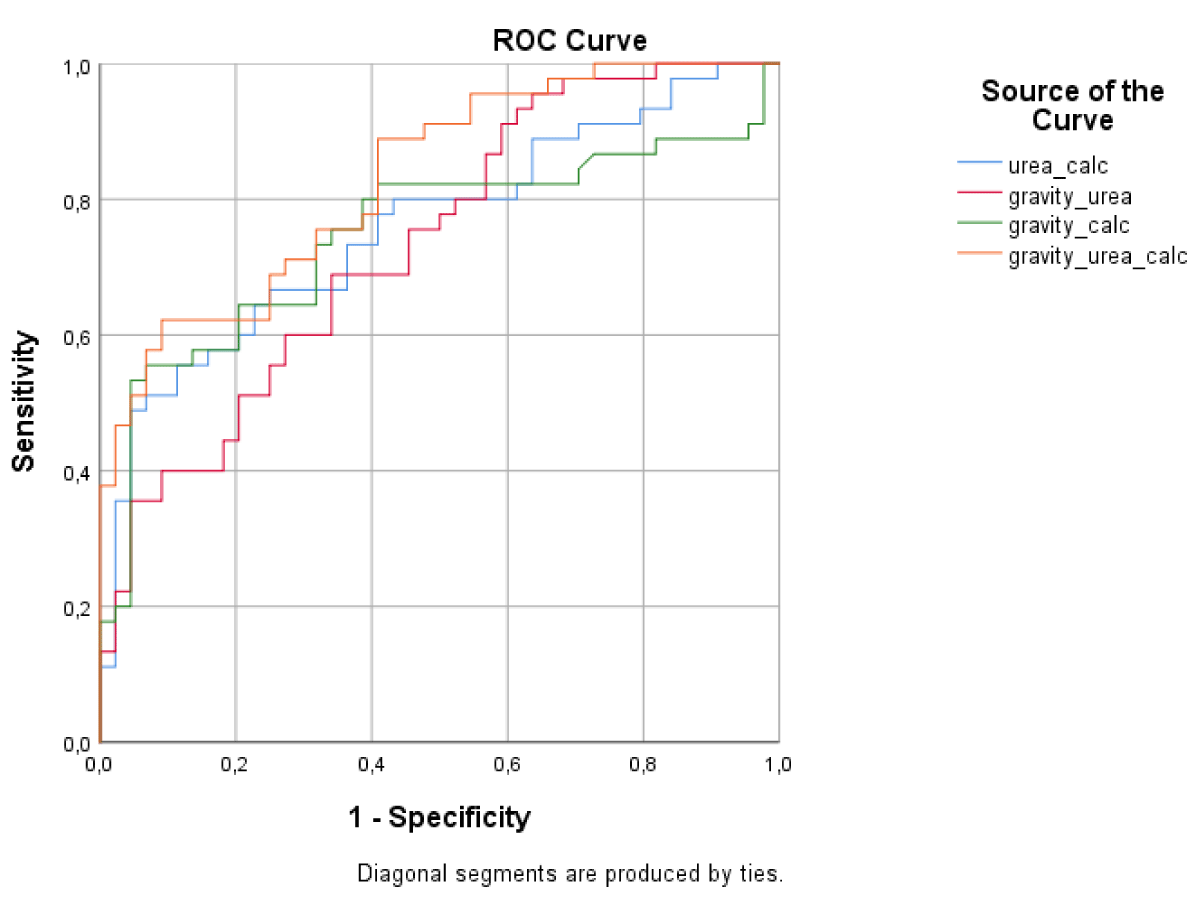
Figure 2: Graph of ROC analysis results for combinations.
| Table 5: Result of ROC analysis for combinations. | |
| Test Result Variable(s) | Area Under the Curve (AUC) |
| gravity_urea | 0.734 |
| gravity_calc | 0.746 |
| Urea_calc | 0.759 |
| gravity_urea_calc | 0.831 |
In the ROC analysis for the combinations, it was observed that the urea variable, which had the lowest discriminative power in the single ROC analysis, increased its discriminative power when considered together with gravity (AUC = 0.734). Likewise, when analyzed with the calc variable, the discrimination power increased (AUC = 0.759). Finally, when the 3 variables with discrimination power are considered together, it is seen that this combination discriminates the target variable, kidney stone, and more (AUC = 0.831).
Kidney stones are highly prevalent, affecting approximately 10% of adults worldwide, and the incidence of kidney stone disease is increasing day by day. An imbalance of crystallization inhibitors and promoters is implicated in the formation of kidney stones. The underlying etiology of kidney stone formation in most patients has been reported to be multifactorial. These factors include environmental, dietary, hormonal, and genetic components [15]. The rising prevalence and increasing recurrence rates of kidney stone disease worldwide can be attributed to limited effective drug options [16]. Kidney stones can affect all ages, genders, and races [3,17]. However. the incidence is higher in men aged 20-49 years than in women [18]. The recurrence rate of secondary stone formations is estimated to be 10% - 23% per year, 50% in 5-10 years, and 75% in 20 years if patients do not perform metaphylaxis [17]. However, although the incidence of kidney stones is increasing in women, the recurrence rate is higher in men than in women. Therefore, prophylactic treatment is very important in the management of kidney stone disease [19]. Extensive studies in recent years show that the disease is on the rise due to lack of physical activity, dietary habits, global warming and lifestyle changes, and the disease is on the rise in both developed and developing countries [3,20,21].
The economic burden of renal failure, which creates a significant disease burden with the severe pain it causes in patients, is quite large. Considering both the direct and indirect costs associated with the disease, annual expenditures for the disease are quite high for all countries. Therefore, preventing the formation of kidney stone disease or reducing recurrence rates is very important for the health sector and patients. In this context, various studies that comprehensively analyze the risk factors of the disease are needed and it is important to address the risk factors associated with the disease more comprehensively. Within the scope of this study, in addition to examining the individual contributions of some factors associated with kidney stones to the disease, how these variables will affect kidney stones when taken together and their effectiveness in differentiating the disease will be examined.
According to the results of statistical analysis, statistically significant differences were obtained for gravity and calc variables for the presence and absence of kidney stones. Gravity and calc variables were found to increase in the presence of kidney stones. In addition, according to the logistic regression analysis using the backward variable selection method, gravity, cond, urea, and calc variables were found statistically significant.
The results of the ROC analysis were performed to examine their discrimination in the case of kidney stones for the variables calc, urea, gravity, and cond, which were found to be significant in the logistic regression analysis, were obtained as AUCcalc = 0.746. AUCurea = 0.602. AUCgarvity = 0.713 and AUCcond = 0.509. An AUC greater than 0.9 indicates excellent diagnostic yield. An AUC between 0.7 and 0.9 indicates good diagnostic yield, while an AUC between 0.5 and 0.7 indicates poor diagnostic yield, and finally, an AUC of not more than 0.5 indicates that the marker has no diagnostic value. According to the classification made for AUC. The cond variable cannot distinguish kidney stone status. The other 3 variables gravity, urea, and calc can differentiate the disease.
As a result of ROC analysis, combinations of variables with discriminatory power were taken to examine their contributions together. Combination made: gravity and urea; gravity and calc; gravity, urea, and calc. When the results of the ROC analysis using combinations are examined, it is seen that the urea variable, which has the lowest discrimination feature in a single ROC analysis, increases its discrimination power when considered together with gravity (AUC = 0.734). Likewise, when analyzed with the calc variable, the discrimination power increased (AUC = 0.759). Finally, when the 3 variables with discrimination power are considered together, it is seen that this combination discriminates the target variable, kidney stone, and more (AUC = 0.831).
One study showed that the prevalence of kidney stones increased with increasing urine-specific gravity [22]. In another study, a steadily increasing stone formation was also observed with increasing specific gravity [23]. In one study, it was shown that urea was excessive in kidney stone patients with uric acid stones [24]. In a study, it was mentioned that the role of electrical conductivity (cond) and total dissolved solids in the formation of urinary crystals is not well discussed in the literature and these variables were examined [25]. Another study aimed to develop an electrical conductivity (EC) measurement system from urine samples to assess the risk of kidney stone formation [26]. As a result of the studies, it was seen that the variables used in the analyses were the variables examined in kidney stone formation. The results of the present study also support the literature.
In light of the findings obtained in the study, it can be said that the variables associated with kidney stones individually have limited power to distinguish the disease, and high accuracy in diagnosis can be achieved by considering the factors associated with the disease together in the diagnosis of the disease. In addition, it can be said that the diagnostic accuracy to be obtained with only one variable for kidney stones may be limited and it is important for the patient to evaluate some parameters together for a definitive result and to start treatment by obtaining a definitive result in terms of the progression of the disease. The high cost of the disease can be reduced by avoiding unnecessary treatment in patients with a definitive diagnosis.
- Alexander RT, Hemmelgarn BR, Wiebe N, Bello A, Morgan C, Samuel S, Klarenbach SW, Curhan GC, Tonelli M; Alberta Kidney Disease Network. Kidney stones and kidney function loss: a cohort study. BMJ. 2012 Aug 29;345:e5287. doi: 10.1136/bmj.e5287. PMID: 22936784; PMCID: PMC3431443.
- Morgan MS, Pearle MS. Medical management of renal stones. BMJ. 2016 Mar 14;352:i52. doi: 10.1136/bmj.i52. PMID: 26977089.
- Romero V, Akpinar H, Assimos DG. Kidney stones: a global picture of prevalence, incidence, and associated risk factors. Rev Urol. 2010 Spring;12(2-3):e86-96. PMID: 20811557; PMCID: PMC2931286.
- Wang Z, Zhang Y, Zhang J, Deng Q, Liang H. Recent advances on the mechanisms of kidney stone formation (Review). Int J Mol Med. 2021 Aug;48(2):149. doi: 10.3892/ijmm.2021.4982. Epub 2021 Jun 16. PMID: 34132361; PMCID: PMC8208620.
- Xu CJ, Li D. Pharmacokinetics of 2-hydroxyflutamide, a major metabolite of flutamide, in normal and CCl4-poisoned rats. Zhongguo Yao Li Xue Bao. 1999 Jul;20(7):655-8. PMID: 10678134.
- Zeng G, Mai Z, Xia S, Wang Z, Zhang K, Wang L, Long Y, Ma J, Li Y, Wan SP, Wu W, Liu Y, Cui Z, Zhao Z, Qin J, Zeng T, Liu Y, Duan X, Mai X, Yang Z, Kong Z, Zhang T, Cai C, Shao Y, Yue Z, Li S, Ding J, Tang S, Ye Z. Prevalence of kidney stones in China: an ultrasonography based cross-sectional study. BJU Int. 2017 Jul;120(1):109-116. doi: 10.1111/bju.13828. Epub 2017 Mar 21. PMID: 28236332.
- Heers H, Turney BW. Trends in urological stone disease: a 5-year update of hospital episode statistics. BJU Int. 2016 Nov;118(5):785-789. doi: 10.1111/bju.13520. Epub 2016 May 26. PMID: 27128735.
- Scales CD Jr, Smith AC, Hanley JM, Saigal CS; Urologic Diseases in America Project. Prevalence of kidney stones in the United States. Eur Urol. 2012 Jul;62(1):160-5. doi: 10.1016/j.eururo.2012.03.052. Epub 2012 Mar 31. PMID: 22498635; PMCID: PMC3362665.
- Stamatelou K, Goldfarb DS. Epidemiology of Kidney Stones. Healthcare (Basel). 2023 Feb 2;11(3):424. doi: 10.3390/healthcare11030424. PMID: 36766999; PMCID: PMC9914194.
- Ziemba JB, Matlaga BR. Epidemiology and economics of nephrolithiasis. Investig Clin Urol. 2017 Sep;58(5):299-306. doi: 10.4111/icu.2017.58.5.299. Epub 2017 Aug 10. PMID: 28868500; PMCID: PMC5577325.
- Eisner BH, Goldfarb DS. A nomogram for the prediction of kidney stone recurrence. J Am Soc Nephrol. 2014 Dec;25(12):2685-7. doi: 10.1681/ASN.2014060631. Epub 2014 Aug 7. PMID: 25104802; PMCID: PMC4243365.
- Tzelves L, Berdempes M, Mourmouris P, Mitsogiannis I, Skolarikos A. Optimal Delivery of Follow-Up Care for the Prevention of Stone Recurrence in Urolithiasis Patients: Improving Outcomes. Res Rep Urol. 2022 Apr 19;14:141-148. doi: 10.2147/RRU.S277498. PMID: 35469244; PMCID: PMC9034870.
- Brikowski TH, Lotan Y, Pearle MS. Climate-related increase in the prevalence of urolithiasis in the United States. Proc Natl Acad Sci U S A. 2008 Jul 15;105(28):9841-6. doi: 10.1073/pnas.0709652105. Epub 2008 Jul 14. PMID: 18626008; PMCID: PMC2474527.
- Tundo G, Khaleel S, Pais VM Jr. Gender Equivalence in the Prevalence of Nephrolithiasis among Adults Younger than 50 Years in the United States. J Urol. 2018 Dec;200(6):1273-1277. doi: 10.1016/j.juro.2018.07.048. Epub 2018 Jul 27. PMID: 30059688.
- Singh P, Harris PC, Sas DJ, Lieske JC. The genetics of kidney stone disease and nephrocalcinosis. Nat Rev Nephrol. 2022 Apr;18(4):224-240. doi: 10.1038/s41581-021-00513-4. Epub 2021 Dec 14. PMID: 34907378.
- Knoll T. Epidemiology, pathogenesis, and pathophysiology of urolithiasis. European urology supplements. 2010; 9(12): 802-806.
- Moe OW. Kidney stones: pathophysiology and medical management. Lancet. 2006 Jan 28;367(9507):333-44. doi: 10.1016/S0140-6736(06)68071-9. PMID: 16443041.
- Edvardsson VO, Indridason OS, Haraldsson G, Kjartansson O, Palsson R. Temporal trends in the incidence of kidney stone disease. Kidney Int. 2013 Jan;83(1):146-52. doi: 10.1038/ki.2012.320. Epub 2012 Sep 19. Erratum in: Kidney Int. 2013 May;83(5):972. PMID: 22992468.
- Alelign T, Petros B. Kidney Stone Disease: An Update on Current Concepts. Adv Urol. 2018 Feb 4;2018:3068365. doi: 10.1155/2018/3068365. PMID: 29515627; PMCID: PMC5817324.
- Robertson WG, Heyburn PJ, Peacock M, Hanes FA, Swaminathan R. The effect of high animal protein intake on the risk of calcium stone-formation in the urinary tract. Clin Sci (Lond). 1979 Sep;57(3):285-8. doi: 10.1042/cs0570285. PMID: 573189.
- Sofia NH, Walter TM, Sanatorium T. Prevalence and risk factors of kidney stone. Global Journal for Research Analysis. 2016; 5(3): 183-187.
- Mao W, Zhang H, Xu Z, Geng J, Zhang Z, Wu J, Xu B, Chen M. Relationship between urine specific gravity and the prevalence rate of kidney stone. Transl Androl Urol. 2021 Jan;10(1):184-194. doi: 10.21037/tau-20-929. PMID: 33532308; PMCID: PMC7844516.
- Chen Y, Roseman JM, Funkhouser E, DeVivo MJ. Urine specific gravity and water hardness in relation to urolithiasis in persons with spinal cord injury. Spinal Cord. 2001 Nov;39(11):571-6. doi: 10.1038/sj.sc.3101209. PMID: 11641806.
- Manzoor M, Mujeeburahiman M, Rekha P. Association of Serum Biochemical Panel with Mineralogical Composition of Kidney Stone in India. Acta Medica International. 2017; 4(2): 26-30. doi:10.4103/ami.ami_24_17
- Fazil Marickar YM. Electrical conductivity and total dissolved solids in urine. Urol Res. 2010 Aug;38(4):233-5. doi: 10.1007/s00240-009-0228-y. Epub 2009 Nov 17. PMID: 19921168.
- Chung WY, Ramezani RF, Li CH, Tsai VF, Mayeni M. Development of Low-voltage Urine Sample Conductivity Measurement System for Kidney Stone Risk Assessment. Paper presented at the 2021 IEEE 3rd Eurasia Conference on Biomedical Engineering, Healthcare, and Sustainability (ECBIOS). 2021.